Step 1: The roots of the skin cancer may extend beyond where visible. If these roots are not removed, the cancer could recur. | 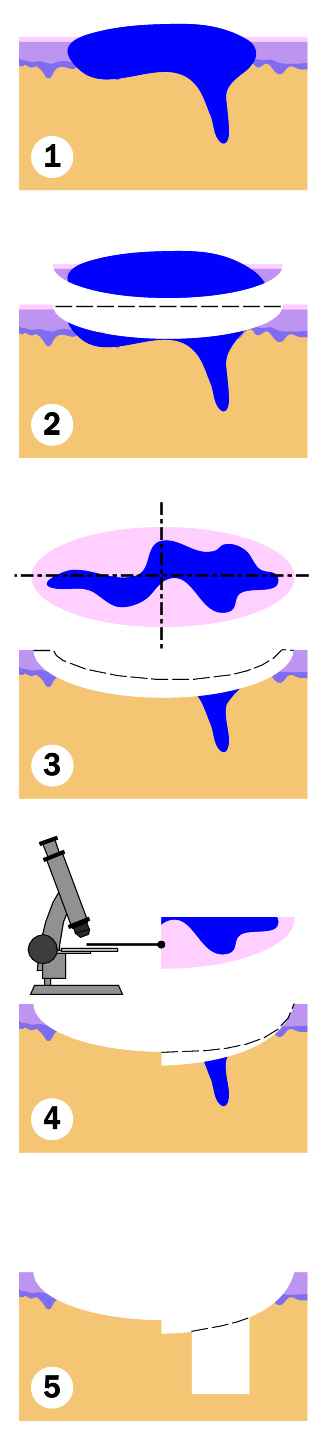 |
Step 2: A layer of skin is removed surgically with a 1-2 mm margin. | |
Step 3: The physician divides the tissue into sections and then color codes the sections with dye. Reference marks are made on the skin to orient the sections. A map of the surgical site is then made. | |
Step 4: The entire base of the specimen is examined microscopically for evidence of remaining cancer. If remaining cancer cells are found, another layer of skin will be removed precisely where cells were seen according to the map. | |
Step 5: Once there is no longer evidence of cancer cells, a surgical reconstruction of the site is completed. |
Mohs surgery is named after Dr. Frederic Mohs who developed this specialized treatment for the removal of skin cancer. This method differs from other methods of treating skin cancer by using complete microscopic examination of the margin of surgically removed tissue and detailed mapping techniques that allow the surgeon to track and remove all extensions of the skin cancer. Mohs is a staged processing technique that offers an alternative to standard excision techniques, and that has been shown to be the most effective method to completely remove skin cancers.
There are two basic steps to each Mohs Micrographic Surgery stage. First, a layer of tissue is surgically excised with a narrow margin around the clinically evident tumor or biopsy site, and at an appropriate depth below the tumor in an effort to completely excise the tumor. Next, the tissue is processed using a method called fresh frozen sectioning and prepared for examination underneath the microscope. On the microscopic slides, Dr. Toner will examine the entire margin of the cut specimen including the bottom surface and the outside cut edges processed into the same plane. During the collection of the tissue the surgeon also marks the specimen so as to orient the specimen relative to the defect on the patient. If any tumor is seen during the microscopic examination, its location is established and an additional corresponding thin layer of tissue is excised from the involved area. The microscopic examination is then repeated as necessary to obtain clear surgical margins. Mohs surgery allows for the selective removal of the skin cancer, while preserving as much of the surrounding normal tissue as possible. Due to the effectiveness of the techniques utilized in Mohs surgery, there is a 97-99% chance for complete removal without an excessive loss of normal tissue.
After the cancer is removed, a decision is made for the best method of repairing the wound created by the surgery. Most frequently, the wound is closed with stitches in a side-to-side fashion, by a skin graft, or by a skin flap. Occasionally, when the wound is small enough or in select locations on the face, no stitches are required, and the wound can heal on its own. Most patients will not require further procedures after the repair of the surgical defect. Very rarely, some repairs are completed in two stages, with the second stage occurring two to three weeks after the initial surgery. After the surgery is completed, the patient is then seen for a wound check or suture removal one week from the date of their surgery. Dr. Toner sometimes will see the patient again for an additional post-operative evaluation.
Infrequently, a tumor may turn out to be much larger than anticipated. Under these circumstances, reconstruction may require another specialist. This surgery may take place on the same day or on a subsequent day. It is very rare that reconstruction may require hospitalization.
About skin cancer
Skin cancer is the most common malignant tumor in humans, and is most commonly found as either basal cell carcinoma or squamous cell carcinoma. These two types of skin cancers have a few variations in diagnosis such as infiltrative basal cell carincoma and squamous cell carcinoma in situ. Both basal cell and squamous cell carcinomas begin as a single point in the upper section of the skin and slowly enlarge, spreading both along the surface and downward. These extensions cannot always be directly seen. The tumor often extends beyond what is visible on the surface of the skin. If not completely removed, both types of skin cancer may invade and destroy structures in their path. Although these skin cancers are locally destructive, they do not tend to metastasize (spread) to distant parts of the body. Squamous cell carcinoma is slightly more risky in certain settings and patients should be assessed periodically by a general dermatologist for any recurrence of the tumor. These types of cancers are best treated by Mohs surgery, especially ones that are on the head and neck. They can generally be resolved in a single visit with Dr. Toner including the reconstruction of the wound resulting from the removed cancer.
Less common but potentially more lethal is malignant melanoma which is generally handled by an excision, not using Mohs surgery, and with a delayed repair. You would have an appointment to have the tumor removed and we would have you come back in a week, after the pathology report has been finalized, in order to complete the repair. This method delayed repair, until it is clear that the cancer has been removed as determined by the pathology report. Once it has been confirmed that the margins are clear, the reconstruction will be completed by Dr. Toner.